MEDICAL INSURANCE PRACTICE
Author: Dimitar Nikolov; translated in Bulgarian
Editor's Note: This is not the first instance we have been commenting on the genesis of medical insurance in Bulgaria. Somewhat awkward we tried in our unpublished manuscript (2002) to present data on the "Fund for Social Security" /FSS/ which functioned at the "Ministry of Trade, Industry and Labor" until 1944. But this attempt was inadequate in terms of literature sources and international comparisons. Recently we got access to some new materials concerning insurance policies in Bulgaria during the inter-war period — viz., the works of Dimitar Nikolov, a lawyer with specialization in social insurance at the International Labor Organization. Interestingly and because insurance practice was at its heyday in Germany, England and other countries, authors like D. Nikolov counted on mainly translated and foreign literature for their compilations. Thus a good source in English language could, eventually, give a viable picture for the state of affairs in Bulgaria. In this particular case for medical insurance and the article from Alfred Cox on the NHS in England (1901-1948) has become a best paragon for theoretical introduction in the subject. Beware one thing only, since, functionary of a Ministry of Health and underlying issues at debate couldn't have been possible in a country like Bulgaria because women suffrage here was banned until 1938. From this standpoint England has remained pioneer state in the introduction of medical insurance practice worldwide, ditto.
Medicine and the State, 1901-1948
The connection between the health of the individual and that of the body politic was not a new insight at the turn of the 20th century but it was one that had began to compel political activity by the state in redrawing the boundary between the public and private in medicine. A century before this the caricatures of Gillray, Cruikshank and Rowlandson had deployed a visual metaphor in lampooning the parlous state of the political nation through depicting sick and dying patients in the care of impotent doctors. By 1904, however, the findings of the International Committee on Physical Deterioration had given a new political imperative to this analogy in indicating that the vigor of the imperial state depended upon the physical health and well-being of the individual citizen.
Although it has been alleged that "most medical histories have devoted little attention to the state", it would be more accurate to say that attention has been focused on the state at moments of high policy — the 19th century incursion into public health (PH), the 20th century inception of national health insurance (NHI), or the national health service (NHS) — whilst intervening periods have been neglected. This chapter will concentrate on the role of interest groups, and on the contrasting impact of provider and consumer groups, in shaping the state's growing interventionism between the end of the Victorian era and the beginning of the NHS in 1948. Within this intervening period there was a transition from the belief that the private medical market was the most effective deliverer of health care to the view that it was the state that could do so more efficiently. In heath there was also some blurring of the public / private divide; state intervention into the family and the so-called private sphere was counterbalanced by private interest groups which became involved with the state in corporate decisions.
Health became a major responsibility of the state in 1948, yet the NHS had been created form a complex of pre-existing services, both public and private. The state had entered the field of health, as of the social services more generally, because of: (i) the charitable urge to help out people in suffering or distress; (ii) the social motive of setting minimum standards of education, hygiene, medical treatment and so on in the interests of the community; (iii) the democratic tendency towards reducing inequalities of status and opportunity; and (iv) the "self-help" philosophy of encouraging or compelling people, by schemes of organized thrift, to protect themselves against risks to which they are exposed.
Variations and inequalities in local services resulted from the decentralized system of the 19th local state. Laissez-faire attitudes, together with the availability of those administrative work-horses that the poor-law guards, meant that it had been expedient for central government to devolve public responsibilities on to local bodies. This had also been facilitated by the activism of municipalities in public health, as was shown by the growth of medical officers of health (i.e., from fifty in 1870 to about two-thousand some thirty years later) and by their contemporary activity in providing sewerage and piped water supplies. Before 1901, therefore, much of the responsibility for social medicine was borne locally rather than nationally. This balance between centre and locality began to change with the NHI of 1911, and there was a more obvious administrative dualism between community services and social insurance. Considerations of public safety, of economic efficiency and of equity were prominent in shaping the first, while the social spreading of risk was more obviously important in the second. The creation of the NHI was intimately related to German precedents and therefore with "great power" competition to achieve a healthy and economically productive people. Significantly the NHI was also related to a desire to delimit state involvement financially by giving the state a mainly regulatory function. The NHI scheme was thus restricted and its limited benefits were conferred principally on lower-paid, employed adult males.
Even before the advent of NHI the confusion of uncoordinated medical services had been well documented in the Minority Report of the Royal Commission on the Poor Laws of 1909. It recommended a unification of the preventive and medical services of the poor law and the public health services of local authorities. Community services at this time included: 1) the notification and control of infectious diseases, 2) TB service, 3) industrial health, 4) mental disorders, 5) mental deficiencies, 6) maternal and infant welfare, 7) school medical service, and 8) provision of clean water supply and efficient sanitation. Involved in their administration were three government departments, and numerous other bodies including boards of control, and over 1500 county, borough and district councils. This inchoate structure potentially gave multiple possibilities in devising a national health service, so that an interpretation of the health system as possessing an obvious hierarchic regionalism in structure — within an inter-war context where there was a contemporary consensus on the obvious correctness of these hierarchies of services in geographic regions — is misconceived. Greater insight was shown by George Godber (i.e., a distinguished post-war Chief Medical Officer), in thinking that the NHS marked the transition from, "a mixture of private and gap-filling public services to a system of care which set out to meet all needs".
In evaluating the boundary of the state and the significance of public interventions, further the extent of private medicine was of obvious importance. Private medical care for individuals from the middle and upper classes was the staple of medical practice. The public provision of primary care, in the form of a panel system financed through NHI, was a belated recognition that medical fees were financially outside the reach of the majority of the working class. A voluntary health sector of the population, on the contrary, was increasingly providing treatment for the more affluent in return for payment.
An important actor in the eventual transformation of this great variety of medical services into the NHS was the Ministry of Health. Its creation in 1919 was interpreted over-optimistically by its inter-war Chief Medical Officer as implying, "a new sort of attack on the strongholds of disease, increased intervention by the state, the betterment of the environment, a higher degree of coordination of national and municipal agencies". But the new ministry was also responsible for local government and for agencies dealing with poverty, and therefore was split between those ideological dinosaurs who adhered to the traditional poor law mentality of economy and delimitations, and those with a more progressive attitude towards the people's health. The influence of the first group was buttressed by strong National Treasury pressure which brutally constrained government spending during the economically depressed 1920s and 1930s. These circumstances also tended to favor the interests of provider groups as against consumer-oriented ones. The British Medical Association (BMA) has been interpreted as becoming at that time "the creature of public medical policies engaged in constant co-operation with the Ministry of Health". This meso-corporatism, where a more powerful professional group defended a sector monopoly interest against weaker consumer interests, meant that politics became medicalized and medicine politicized.
***
Doctors as providers, or the panel system
This medical corporatism involved the Socialist Medical Association, the Medical Practitioners Union and the BMA, but attention is confined here to the largest group — the BMA. Already in 1901 it represented half of all doctors on the Medical Register and this had risen to three-quarters by 1948. These were general practitioners (GPs) rather than the elite of the profession — the specialists and consultants. The BMA was male dominated. Women were in a small minority in the medical profession and even by 1937 they comprised only 11 % of its members. The BMA became politically active, clashing with government at moments of high policy at the start of the NHI and NHS, but also becoming enmeshed more continuously, although less visibly, with the state in its administration of a growing range of public medical services. It was a source of technical medical knowledge, a liaison agency and a means of mobilizing GPs involvement in state policies. Thus, the BMA has been interpreted as being a "vital part of the departmental decision-making". Another assessment suggests the importance of doctors as decision-makers in the creation of the NHS; civil servants, however, neither understood GPs and the BMA nor were able to match their influence.
Within this framework of received interpretation and what were the successes of the providers interest group — the BMA? Doctors' remuneration was at the top of its agenda. As inherently noticed, "the unnerving discovery every Minister of Health makes is that the only subject he is ever destined to discuss with in the medical profession is money". An important indicator of the power of an interest group is its ability to get resources for its members, but on this measure BMA does not score highly. In 1911, the GPs were given an economic windfall of sizeable proportions by the state in the NHI scheme. This generosity was largely because the state was unaware of the low incomes and underemployment of many medical practitioners at that time. Since the BMA was also ill informed on this critical point, subsequently, it opposed what it perceived as an offer of inadequate remuneration. Thus it was unable to carry a major section of the profession with it and ended up bereft of credibility, having to ratify what individual members had already decided to do through joining the panel system. During the inter-war period the BMA was ineffectual in its attempts to raise state payments to panel doctors. GPs found that state payments were declining elements in their income, and that a shrinking proportion of their total income came from public funds, which decreased from one-half in 1922 to one-third by 1938. Powerful economic pressures were operating in crisis years to curtail state expenditures still further so that panel doctors' capitation fees were reduced by 10 % in 1931-4, and by 5% in 1934-5. Thus, whilst panel income was a useful adjunct to income from private practice, it was the private rather than the public component that was buoyant, and that enabled GPs to do better than their other professional colleagues.
The panel system institutionalized an existing tension between doctor and patient in that the state emphasized the the quantity of care delivered rather than intervening to improve its quality. It tended to encourage routine procedures linked to a low standard of patient care; engaged with over-prescription; showed reluctance to treat difficult cases rather than to refer them elsewhere; and tolerated an under-investment in modern equipment and premises. In lengthy negotiations between the state and the BMA remuneration was a central concern and health-related matters usually peripheral. The Secretary of the BMA did write to the Minister of Health given this socio-economic disadvantages. But the position of the Ministry was centered on the promotion of positive health rather than the treatment of disease. This were the kernel issues that further transposed to the campaigns of the women's organizations.
***
Women as consumers, or the equity scheme
This section looks at women's consumer interest groups in relation to the state and medicine, at a time when the state's incursion into health was very obviously benefiting certain sectors of the male population. For example, some studies concluded that the working classes were very important as a consumer interest groups in relation to the NHI, but in discussing a scheme that was designed for the lower-paid male worker failed to explore its gender dimension. Yet health has been central to the emancipation of women whether as citizens possessing political rights, as consumers and clients of welfare services, or as employees. However, their involvement in the extension of the state's boundary in relation to health was a complicated one, and the focus of their interest groups was not only the NHI but more general policies related to maternal and infant welfare.
Earlier feminist analyses of more advanced or fully developed welfare states drew attention to the fact that women had less power in the labor market than men, and hence less opportunity to defend or consolidate their position in the political system through interest groups. In this interpretation women were perceived as difficult pertaining to finding integration into the political system and participation in the decision-making process. It was said that health policies in Britain were formulated before women had the suffrage (i.e., in 1918 and 1928) and thus that women found themselves mainly as the objects, or consumers, of policies and public interventions that they had had little opportunity to shape. In their attempt to influence policy-making in maternal and infant welfare, women were seen as having been penalized both by their late arrival on the political scene, and by more deep-seated structural factors. In a significant discussion of the long-term basis of the modern patriarchal state, contemporary authors argued that there were intractable problems in contractual theory concerning women's incorporation into civil society since that was a strong influencing factor on people's health. Health had become an important function of the poor law and from the mid-1870s the Women's Cooperative Guild (WCG) had campaigned for working-class women to come forward. In the field of maternal and infant health questions were posed like, "Would women like men choose their own nurses, inspect their own sickrooms and their nurseries?" Women guardians had taken a particular interest in improving workhouse sick wards, and pressurizing the state into making more effective use of trained nurses there. In public health, too, women had been conspicuously active, although by the early 20th century an earlier role of female sanitary inspector was being superseded by less well-paid health visitors. Women councilors' work in the early 20th century was centered on the issue of infant mortality, and by 1918 their energy, together with voluntary work by many other women, had assisted in the creation of nearly a thousand maternity and infant clinics. Other factors were also of importance, not least the appreciation in time of war of the importance of infant lives to replace casualties, so that the Local Government Board made several amendments in infant and maternal law. Women's organizations were therefore pushing with the tide and the successful implementation of their objectives in 1918 owed much to this. Indeed, these early nurseries-clinics on municipal level were aptly described as a "form of war-work".
"We feel we can congratulate ourselves on the formation of these Municipal Committees. Work formerly done by voluntary societies is now being taken over by the municipality", commented the WCG on the Maternity and Infant Welfare Act of 1918. The WCG had helped bring about this outcome by producing leaflets such as "What Health Authorities Can Do" and Municipal Maternity Centers", and had also published the moving "Maternity Letters" in 1915, accounts of the experiences of maternal ill-health and over-work among guild members. The Women's Labor League also campaigned forcefully for this legislation. The act of 1918 allowed municipalities to provide clinics, salaried midwives, nurseries, food and milk for the poor, etc. Thus the actual work of the "sense of sex grievances, was developed into a sense of sex solidarity". What were the health issues that this solidarity produced?
Uniquely among compulsory insurance schemes the NHI had excluded dependants, and in 1926 the Royal Commission on Health Insurance dismissed the idea of including dependents because the cost would be "prohibitive". There was strong pressure from women's organizations for a more comprehensive system that paid due attention to their needs. Initially, woman's organizations had been horrified to find that the 30 shillings maternity benefit in the scheme for the wives of insured men, for which they had campaigned so hard, was to be paid not to women but to men. As a result of a vigorous campaign this was altered and it was acknowledged to be the legal property of women. What the maternity benefit meant in practice was explained to women by Selina Cooper, appointed as one of the trained nurses by the official National Insurance lecturers. Cooper also made suffrage propaganda out of the act saying, "The Insurance Act affects women just as much as men, and they have to contribute 3d per week equally with men. But the men have the option of voting either for or against the Act, and the women have not".
In 1915 the most well-established female pressure group, the WCG, campaigned for a national scheme that would combine "administration of benefits under the Insurance Acts with the services organized by the Public Health Authority". It wanted a Ministry of Health with a "Maternity and Infant Life Department" providing: 1) extended maternity and pregnancy benefits, 2) status of health visitors elevated to that of women health officers, and improved and salaried midwifery service, 3) maternity and infant centers, 4) increased number of maternity homes and hospitals, 5) municipal milk depots, 6) provision of household helps for women around the time of childbirth, 7) more women councilors, and women represented to a much greater extent on public health committees. A more active intervention role by the state in health was also the object of campaigns by the National Union of Societies for Equal Citizenship and the Women's Freedom League. The latter stated that, "Women are angry because of the perpetual dallying of the authorities in regard to the establishment of a Ministry of Health".
Once a Ministry of Health has been set up in 1919 and women criticized its arrangements and especially its linkage of health with poor-law administration. The WCG resolved that there ought to be a thorough investigation and with a desired outcome of a state medical service unconnected with the poor law. Earlier, the medical correspondent of Times had suggested that, "The underlying idea of a Ministry of Health is to cement the alliance between the mother and the doctor". This was an unrealistic view since it ignored the tensions between their interests, but one of the few promising signs of collaboration was a "Consultative Council on General Health Questions" which was set up in 1919 with Lady Rhondda in the chair and with a majority of female members. That it had no discernible impact on state policy was a bad omen. Subsequently, the Ministry was a convenient target in attempts to reform NHI and some pertinent objections were made to the gender biases of insurance schemes: women were penalized by being treated alongside the men in unemployment schemes (i.e., because women had fewer claims), but in health insurance where they had more claims they were separated. Women MPs took exception to the official perception that married woman's sickness claims under NHI were "excessive" and that malingering had taken place. How could the state really wish to improve maternal welfare, they argued, when Parliament gave a higher priority to actuarial soundness in the NHI scheme, thus reducing women's benefit rates. Miners, they pointed out, also had high sickness rates but suffered no corresponding penalty.
During the inter-war period women had low citizen status with few women representatives in the House of Commons. The first woman MP had been elected in 1918, numbers in the inter-war period reached a highpoint of fifteen in 1931, and a further increase was made to twenty-four in 1945. Women believed that if they could gain greater power within the central state they would be able to influence health policy. The Women's Freedom League made the demand "that there shall be a woman Minister of Health, appointed from women members elected to the House of Commons". A decade later, in 1929, Susan Lawrence, a Labor MP, became the next best thing as Parliamentary Secretary to the Ministry of Health, and was supported by a parliamentary majority.
This state of affairs had been lingering for quite some time (i.e., imminent in mid-1950s) and the extent to which unequal gender and social delivery falsified the title of a "national health service" was also evident. This can be linked to a historical concentration of male medical specialists, with a related institutional provision within relatively few geographical areas, and the successful defense of this system until 1948 by the elite doctors safeguarding their interests.
***
Conclusion
In suggesting that "there is no limit to the usefulness of a proper and enlightened co-operation between medicine and the state", C. Addison, the first Minister of Health, had been over-optimistic. Provider interest groups in medicine were more effective negatively (i.e., in defending the status quo), than positively (i.e., in promoting radical changes) in their attempts to shape the NHS. In doing so they had some influence on the boundaries of the state in preserving an element of private health care and retaining a traditional emphasis on individual, rather than on social medicine. It might have been expected that in health, where there is a considerable public interest, professional power would have been more constrained and patient's interests have had more weight. But when patient's interests were represented by women's groups then relatively little success was attained in extending the inter-war boundary of the central state's responsibility. It was striking that women participated as citizens in the NHS, as they had not done universally under the NHI, but this owed more to the transformation effected in social attitudes by war than to earlier activity by consumer pressure groups. In the slow development of a NHS there had been no obvious winners despite continuous activism by both provider and consumer interest groups. Adjustment to democracy in the medical boundaries of the state had been a slow and uncertain process, in which the relationship between the health of the individual and that of the body politic had been related as inherently problematic.
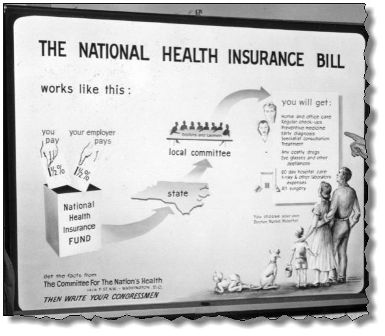
Picture 1: Sample illustration of National Health Insurance Bill.
|
(i). Works like this: You pay 1½ % flat tax rate + Your employer pays 1½ % flat tax rate; You will get, 1) home and office care, 2) regular check-ups, 3) preventive medicine, 4) early diagnosis, 5) specialist consultation, 6) treatment, 7) any costly drugs and other appliances like glasses, 8) 60-day hospital care, 9) x-ray and other laboratory expenses, 10) all surgery, and 11) you choose your doctor, nurse, hospital.
|
Copyright © 2008 by the author.