MANUAL FOR THE FAMILY PHYSICIAN
Author: Ivan Maleev
CLINICAL EPIDEMIOLOGY
In an attempt to predict some of the trends along which Clinical Investigation may proceed in the next few decades, the subject of Preventive Medicine naturally arises as a field for these activities. The term, Clinical Investigation in Preventive Medicine, is cumbersome and so I will not use it. In fact even the term, Preventive Medicine has never seemed ideal. It implies a little too much in the way of propaganda. It presupposes the existence of a so-called sister science, Curative Medicine, and both sciences are committed perhaps too definitely to a therapeutic program. Clinical Investigation in Epidemiology is better for the purposes at hand; Clinical Epidemiology is best, and really what I mean. In fact this is the name I would like to propose for a new science; a new discipline in which this Society might take an important part. It is a science concerned with circumstances, whether they are “functional” or “organic,” under which human disease is prone to develop. It is a science concerned with the ecology of human disease.
But it is more than that, for any science worthy to be qualified by the name Clinical, should involve some attempt at the interpretation of the circumstances with which it deals. It must face the question of “why,” as well as “how.” Clinical Epidemiology differs, therefore, from the orthodox science of Epidemiology both in its aim, and its locale, as it were. The orthodox epidemiologist must of necessity deal dispassionately with large groups of people. It is the multiplication of observations which give him his results. The clinical epidemiologist, on the other hand, must of necessity deal with small groups of people; people whom he knows well and groups no larger than a family, or small community. The restriction of the size of the group rests on the fact that clinical judgment cannot be applied wholesale, without the risk of its being spread too thinly to be effective. Fortunately or unfortunately the amount of personal attention requisite for the exercise of clinical judgment is set by physiological limits which most of us cannot exceed. The clinical epidemiologist, therefore, can dispense just so much of this attention power at one time. He starts with a sick individual and cautiously branches out into the setting where that individual became sick — the home, the family, and the workshop. He is anxious to analyze the intimate details under which his patient became ill. He is also anxious to search for other members of the patient’s family, or community group who are actually, or potentially ill. It is his aim to thus place his patient in the pattern in which he belongs, rather than to regard him as a lone sick man who has suddenly popped out of a healthy setting; and it is also his aim to bring his judgment to bear upon the situation, as well as on the patient.
Obviously there is nothing new to the family doctor about this concept of Medicine. It is the heart and soul of family practice and probably has been, as long as family practice has existed. But now that the emphasis, for this Society at least, has shifted away from the home and into the Hospital and Dispensary, clinical epidemiology will be practiced only if we take thought about it. It is a foreign concept for most intramural clinical investigators whose contact with the actual circumstances under which their patients became ill may be limited to a page in the hospital history, or a supplementary talk with the social worker.
To give a single but well-known example of work in clinical epidemiology which has been accomplished in well-known Institutions in this country, I will name a certain study on the spread of tuberculosis through families. As a contribution to the field of tuberculosis, and also to other infectious diseases this work speaks for itself. But the approach is not limited to Infectious Diseases. It is being used by Dr. Canby Robinson in the study of circumstances which are prone to give rise to a variety of types of illness which bring patients to the Dispensary of the Johns Hopkins Hospital. Clinical epidemiology is also something more than family visits. As an example of another direction, and a most important direction it has taken, are the recent investigations concerned with the pathogenesis of pernicious anemia, and of nutritional deficiencies. In these fields members of this Society have played no small part and may also be said to have already had some share.
The crux of these investigations in the various fields just mentioned lies not only in the discovery of new intrinsic or extrinsic factors, which may be found either indoors or outdoors, but in the discovery of new concepts. The concept of certain new etiological forces which lie back of those which were once thought to be basic, such as for instance, the factors which lie back of the pneumococcus as a cause of pneumonia. This is all so obvious that it hardly seems worth mentioning and yet a dominant thing about some of our present notions of causative factors is that unless they fit into a modern pattern of our own liking they are apt to be overlooked. Of late years conservative opinion does not allow anything to be really considered as “etiology,” unless we can succeed in getting it into a test tube, unless we can precipitate it, and unless we can crystallize it as it were. This is due of course to our current methodology which has perhaps become more of a religion than most of us realize. I think it may have led to a slightly narrow interpretation of clinical investigation on our part, for clinical investigation certainly should be given the opportunity to spread itself up into philosophy, if it will, as well as down into the basic sciences.
Now this is not a plea for more papers describing philosophical concepts of epidemiology, for if they are really important they will find their way into our programs of their own accord without having to be plead for. I only say that we ought not to be frightened by them. We ought not to be frightened by the word clinical investigation in the field of Public Health, or clinical investigation outside the Hospital. For, if we are frightened, then it may be true what our critics say, that we have become so attached to our own pet methods and points of view that we have drifted away from the progressive ideals for which this Society was founded.
But there is still another aspect to Clinical Epidemiology which deals with the meaning of disease. For instance, we may now have to dispel a smoke screen that the folklore of both Preventive Medicine and Curative Medicine has thrown out which consist in a sort of censorship about the meaning of disease, in which there are at least two assumptions. These are: (A) that all disease is bad and hence all attempts to prevent it, or cure it are good, regardless of its cause or the conditions under which it arises; and (B) that disease is something which an unkind fate has put upon us, in other words disease is not of our own making but it comes from elsewhere. It is always the “French disease.” To turn the spotlight of investigation upon these assumptions is the first duty of the clinical epidemiologist. It involves a certain amount of risk, the risk of trifling with religious tenets, and as such of being anti-social. It might be anti-social if we found, for instance, that all disease is not necessarily bad, but that a wise Providence inflicts some one with arteriosclerosis or even tuberculosis as a just reward for his “bad living”; or that children’s diseases are rained upon us as a means of furnishing us not only with specific immunity, but who knows, how much non-specific immunity too, which may be of inestimable value to us in adult life.
It might also be something of a betrayal of our clan if we found that a good deal of illness may be laid at our own feet, that is, illness caused by “ultramodern therapeutics,” viz., the creation of invalidism through overzealous treatment, through meddlesome treatment, and through the whole wretched system of abused sick benefits to which we meekly bow our heads. Although such functional causes of invalidism as these cannot be so easily put into a test tube, and cannot be precipitated or crystallized they are powerful etiological factors, intrinsic in our modern civilization, and responsible for a good deal of preventable illness. Strangely enough they have not yet been regarded (by this Society at least) as a particular legitimate field for clinical investigation. Better to stick to something like bubonic plague for which the blame can conveniently be put on the rats, is a code we have followed too much in the past.
If these fields are eventually to be investigated, it is the man with clinical judgment who can best blaze the trail, for it is the prime responsibility of the clinician to do the work. It is his responsibility far more than that of the Public Health specialist, or the bacteriologist, or the chemist. To do this the clinician will, however, have to adopt a new technique, and a new uniform. Gone is the glamorous role of the microbe hunter for this type of investigation, and in his place all we can see is something like a rank sociologist.
But still more important for the clinical epidemiologist than questions of technique and uniform, is his point of view. From the onset he cannot accept as Galenic truths all the creeds, all the rituals of medical research that the generation just preceding his has professed. He is called upon instead to strike out anew without much in the way of organized backing. But there is nothing really alarming or radical about this. Nor should it require the role of a crusader, at least as far as this Society is concerned. It merely reflects the same type of incredulity about methods of studying human disease, which, if I am not mistaken, was the force which brought this Society into being a generation ago.
***
PRIMARY MEDICAL CARE
For centuries care of the sick and injured had consisted of acts of empathy and love largely conducted by religious orders and financed by charitable contributions. Although providing succor and support, largely for the destitute, they were often poorly run and too frequently harbored more disease than they cured. In many ways they reflected the social culture of their times and places. Over the ages hospitals provided care in every sense of the word and often a place to die. To the possibility or promise of cure they gradually added preventive measures, and most recently rehabilitation. At the pinnacle of the hospital hierarchy are medical schools and their affiliated university hospitals, now called “academic health centers”, that train doctors and other health personnel, conduct fundamental, applied and population-based research. In recent decades a growing number of hospitals have been a source of profit for owners and shareholders while their academic contemporaries struggle to stay afloat financially.
Over several centuries the management of hospitals has been extended from the purview of nuns to nurses, sometimes physicians and more often well-meaning lay administrators. Only in the late twentieth century was formal university training for hospital administrators provided. Initially salaries were negligible to low but they have gradually morphed into those of major corporate entities, as their titles have shifted to CEO. Those of commercial insurance companies are even greater.
Florence Nightingale (1820-1910), the founder of modern nursing, born to a wealthy family and well-connected socially, was horrified with the conditions she found in military hospitals during the Crimean War. She embarked on a life-long crusade to improve the care and accountability of British hospitals. Her writings on management, organization, nursing, health statistics and hygiene are landmarks in the evolution of hospitals and related caring facilities.
In Germany Prince Otto Bismarck (1815-1898), an aristocratic conservative with impeccable right-wing credentials, introduced national health insurance as part of his overall social insurance plan — later used as a model for the Social Security arrangements in the United States. Sir William Beveridge's (1879-1963) report on “Social Insurance and Allied Services” contributed the intellectual foundations for the United Kingdom's National Health Service. An exhaustive report by a Royal Commission in Canada resulted in that country’s national health insurance legislation. Today over 46 million citizens have no health insurance. Most national insurance systems and the U.S. Social Security system have overhead charges of about 3%; commercial firms have overheads of 30% or more.
Systems of care that link the various levels of health care started with the work of Lord Dawson (1864-1945) whose landmark report defined and diagrammed links of care from primary health centers, secondary health centers, teaching hospital and home care. In the United States Henry J. Kaiser, a construction magnate, founded the Kaiser-Permanente Health Plan in the latter part of the twentieth century.
There are three perspectives and venues from which to address health and disease:
— Clinical, one-to-one care of individuals;
— Population, studies of groups and communities;
— Biomedical, laboratory investigations at organ, cellular and molecular levels.
During the 19th and early 20th centuries the first perspective dominated medical thinking and action. The paradigm-shifting discoveries of Koch and Pasteur, for example, with their spectacular results from the study of microorganisms, brought the laboratory to the forefront and emphasized the need for collective public measures to prevent and control infectious disease. Others emphasized the critical roles of poverty, famine, filth, unemployment, poor housing and environmental desecration in the genesis of disease.
With biomedical research in the ascendancy, the population perspective languished until 1916 when the Rockefeller Foundation began a lavish global program that created and funded schools of public health apart from medical schools. Cohorts of health officers were trained and the underlying disciplines of epidemiology, statistics, and even the emerging medically-oriented social sciences were hijacked from medical schools to the new expanding public health schools. Many good things resulted but much was also lost. Medicine focused increasingly on molecular research; both clinical and population health research suffered.
That may be changing as barriers among the three perspectives disappear. To study disease, clinicians are analyzing their practices as networks of primary care doctors pool their data in surveys. Public health officials recognize that clinicians are the first-line of observation and reporting for early detection of pandemics and bioterrorism attacks. Geneticists require populations to assess the impact and transmission of much gene-mediated disease. There is no end to the need for collaboration and “stove-pipe” isolation between the three perspectives will soon be history.
Apart from obvious emergencies, it is symptoms, problems, complaints and questions, not labeled “diseases,” that characterize the initial encounters between patients and physicians. “Symptoms are the language of disease”. You don’t have “it” until a doctor labels “it”! Primary medical care doctors are personal physicians who respond, treat, and manage the great bulk of these initial encounters. They provide comprehensive services to individuals and families over long periods of time, often lifetimes. Primary care physicians accept all comers no matter how frequent or trivial the complaint.
Family physicians, general internists and general pediatricians, and increasingly, nurse practitioners provide the great bulk of primary care. In many countries these arbitrary academic and professional divisions do not exist. Family physicians or general practitioners (a term rarely used now) constitute half or more of their nation’s clinical personnel. They recognize that primary medical care clinicians provide the essential underpinning of any rational, balanced, and cost-effective health care system. Virtually all developed countries recognize this well-documented fact. Thus costly, hospital-based, and error-prone medical system is in urgent need of substantial modification.
Life for primary care doctors has not always been easy and the financial rewards have been modest. All that may change as new practice patterns allow primary care physicians more satisfactory personal and family lives and fee schedules that are more realistic. A physician who is curious about the genesis and natural history of disease and illness, and who enjoys people and tolerates ambiguity would find primary care to be a fascinating and rewarding career.
Statistical concepts and methods are essential for both biomedical and health services research and both health statistics and epidemiology make abundant use of their analytic strategies. For population-based surveys, such as those conducted by the National Center for Health Statistics, the methods used were pioneered by social scientists — and social epidemiology is of increasing importance.
Counting is the “stock in trade” of these endeavors but investigators, clinicians, and managers of all disciplines need to remember that not all that “counts” can be counted. Caring, compassion, and hope cannot be easily counted or measured. Nevertheless, familiarity with health statistics, epidemiology, survey applications and methods is now a requirement for all medical graduates.
Of far greater importance is internalization of the underlying concepts of statistical reasoning such as: bias (in its many forms), randomization, probability, sensitivity and specificity, distinction between efficacy and effectiveness, and above all, the difference between statistical and clinical significance.
Counting the dead initially gave way in the 17th century to recording the “causes” of death, and over the decades, to expanding and diversifying their “labels” based on notions of causality. These too have changed frequently over time, thus giving us the 10th edition of the International Classification of Diseases (ICD-10). To address the need for studying the natural history of initial symptoms, their mutation into disease, and its early prevention, the International Classification of Primary Care was created. Accurate and honest labeling is essential for the production of useful epidemiological and statistical information. However, there still remains doubt about the reliability and validity of some morbidity and mortality survey data.
Epidemiologists initially investigated the origins of infectious disease outbreaks. Now they also focus their efforts on chronic illness, behavioral and societal disorders, and evaluating clinical and population-based interventions and services. Epidemiology developed in medical schools in the 19th century and all epidemiologists were physicians. Then in the early 20th century, schools of public health were created and assumed the primary responsibility for developing modern epidemiology. The pendulum has swung back and most medical schools now have clinical epidemiology units or departments that develop and use epidemiological concepts and methods to study disease, assess treatments and monitor care in hospital, ambulatory and community settings. These venues provide alternatives for young physicians to investigate health problems and services outside the biomedical laboratories and hospitals, and demand for such skills continues to grow.
***
Addendum: Several standpoints are worth noting here. As a Manual of General Practice for medics and non-medics this is first of its kind. The book contains information from the fields of Anatomy, Physiology, Hygiene, Preventive Medicine, Therapeutics, Mother and Child Care, Surgery and First Aid, Physiotherapy, Balneology and Curortology, and others. However, this is not textbook for specialists but is meant for small groups (family) in their everyday routines or some emergencies. As later medical experience evolved in the 1950s and 1960s, some general practitioners registered their work as a separate specialty and thus the Institute of GPs had appeared.
In Bulgaria the history of the discipline has scanty precedents. Beside this book only one other manual dealt with similar contents — viz., "Manual for Samaritan Work" (1947) issued by the Bulgarian Red Cross, and further revised by Verbev, P and Dimchev, D (1969) and Gubev, E and Stephanov, G (1987) as "Reference Book for General Practice". Meanwhile the reformed socialized health care paid little attention to strictly individualistic practices and family physicians were banned from work. There appeared the so called "district physician" based on territorial principle and fixed contingent of patients. Albeit, the terminology of "primary medical care" was developed by World Health Organization and many of the standards from GPs were applied to health policy. Until year 2000 all the settings of primary health care were controlled by the state and financed by NHIF (National Health Insurance Fund).
Back on the early years of disciplinary General Practice. The book at hand was written unambiguously by certified medical doctors. We will talk about the editorial staff later. But it is interesting to apprise some precedent roots of the schematic relationship "patient-doctor". During the Middle Ages and up until end of Reformation in the West, patient care was privilege to a chosen few. Hospitals hardly existed in their conventional sense, charitable societies and nursing were highly underdeveloped and only royalties got what they wanted in terms of qualified medical care. In Bulgaria that was part of the Ottoman Empire, general masses and the disinherited and lawless "rayah" were totally neglected as to aspirations for better health. Good chances for survival were accepted up to 40 years of age, and population statistics for mortality and morbidity was non-existent (i.e., except for the Turkish Salnames or Yearbooks, that contained purely paleographic information). Thus the Medical Folklore of the Bulgarians has retained only limited knowledge for their medical practices — viz., we have mentioned previously on folk healers from the Revival period: Mathey Preobrazhensky and Neophit Kalchev, both from the clergy of various bulgarian monasteries. Then it comes the name of Petar Dimkov "The Healer", who was most popular as doctoring people for 80 years or so in this lands and was fine representative of early non-traditional medicine in Bulgaria.
We shall finish this short commentary with enumerating the staff and qualifications of the authors team for the present publication:
1. Dr. I. Maleev ~ specialist in Internal Medicine and Pediatrics;
2. Prof. S. Angelov ~ Dean of Veterinary Faculty, specialist in Bacteriology;
3. Dr. M. Sophroniev ~ specialist in Surgery, on private practice;
4. Dr. H. Stoychev ~ specialist in Balneology and Internal Medicine;
5. Dr. I. Rachev ~ specialist in Pulmology, Alexander's Hospital;
6. Dr. N. Karev ~ specialist in Skin and Venereal Diseases;
7. Dr. P. Popov ~ specialist in Obstetrics and Gynecology.
/to be continued/
Pictures 1 & 2: Sample illustrations on the text above.
|
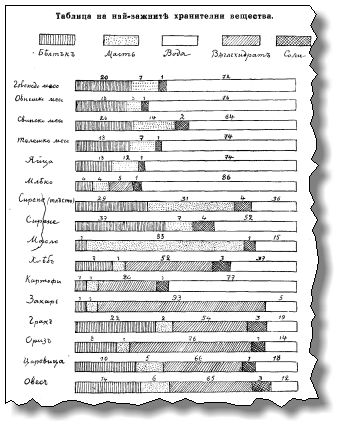
(i). Table of most important nutritional substances contained in various edible food.
|
|
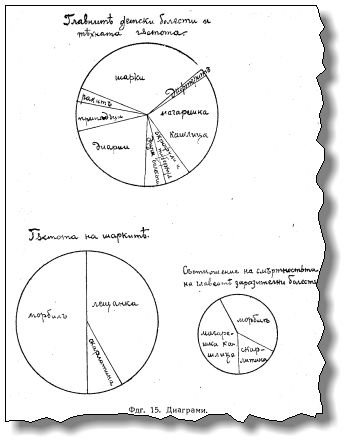
(ii). Diagrams of main infectious diseases prevalence in childhood, their incidence density and lethality index.
|
Copyright © 2010 by the author.